All The Things You Ought To Understand About Heel Aches
Overview

Plantar fasciitis is a painful condition affecting the bottom of the foot. It is a common cause of Heel Pain and is sometimes called a heel spur. Plantar fasciitis is the correct term to use when there is active inflammation. Plantar fasciosis is more accurate when there is no inflammation but chronic degeneration instead. Acute plantar fasciitis is defined as inflammation of the origin of the plantar fascia and fascial structures around the area. Plantar fasciitis or fasciosis is usually just on one side. In about 30 per cent of all cases, both feet are affected. This guide will help you understand how plantar fasciitis develops, how the condition causes problems, what can be done for your pain.
Causes
If it hurts under your heel, you may have one or more conditions that inflame the tissues on the bottom of your foot. When you step on a hard object such as a rock or stone, you can bruise the fat pad on the underside of your heel. It may or may not look discolored. The pain goes away gradually with rest. Doing too much running or jumping can inflame the tissue band (fascia) connecting the heel bone to the base of the toes. The pain is centered under your heel and may be mild at first but flares up when you take your first steps after resting overnight. You may need to do special exercises, take medication to reduce swelling and wear a heel pad in your shoe. When plantar fasciitis continues for a long time, a heel spur (calcium deposit) may form where the fascia tissue band connects to your heel bone. Your doctor may take an X-ray to see the bony protrusion. Treatment is usually the same as for plantar fasciitis: rest until the pain subsides, do special stretching exercises and wear heel pad shoe inserts. Having a heel spur may not cause pain and should not be operated on unless symptoms become chronic.
Symptoms
Plantar fascia usually causes pain and stiffness on the bottom of your heel although some people have heel spurs and suffer no symptoms at all. Occasionally, heel pain is also associated with other medical disorders such as arthritis (inflammation of the joint), bursitis (inflammation of the tissues around the joint). Those who have symptoms may experience ?First step? pain (stone bruise sensation) after getting out of bed or sitting for a period of time. Pain after driving. Pain on the bottom of your heel. Deep aching pain. Pain can be worse when barefoot.
Diagnosis
A podiatrist (doctor who specializes in the evaluation and treatment of foot diseases) will carry out a physical examination, and ask pertinent questions about the pain. The doctor will also ask the patient how much walking and standing the patient does, what type of footwear is worn, and details of the his/her medical history. Often this is enough to make a diagnosis. Sometimes further diagnostic tests are needed, such as blood tests and imaging scans.
Non Surgical Treatment
The following steps may help relieve your heel pain. Use crutches to take weight off your feet. Rest as much as possible for at least a week. Apply ice to the painful area. Do this at least twice a day for 10 to 15 minutes, more often in the first couple of days. Take acetaminophen or ibuprofen for pain. Wear proper-fitting shoes. Use a heel cup, felt pads in the heel area, or shoe insert. Wear night splints. Your doctor may recommend other treatments, depending on the cause of your heel pain. Call your doctor if your heel pain does not get better after 2 - 3 weeks of home treatment. Also call if your pain is getting worse despite home treatment. Your pain is sudden and severe. You have redness or swelling of your heel. You cannot put weight on your foot.
Surgical Treatment
When a diagnosis of plantar fasciitis is made early, most patients respond to conservative treatment and don?t require surgical intervention. Often, when there is a secondary diagnosis contributing to your pain, such as an entrapped nerve, and you are non-responsive to conservative care, surgery may be considered. Dr. Talarico will discuss all options and which approach would be the most beneficial for your condition.
Prevention

You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
The Key Causes And Solutions For Achilles Tendonitis Suffering
Overview
 If you have pain along the back of your leg near your heel, you may have Achilles tendonitis. Achilles tendonitis is an overuse injury that commonly occurs in runners and ?weekend warriors?. The Achilles tendon is the largest tendon in the body. Named after a tragic hero from Greek mythology, it connects your calf muscle to your heel bone to allow you to jump, run and walk. Achilles tendonitis is most common in middle-aged men, but it can happen to anyone who has a sudden increase in physical activity. The risk is increased if you also have tight calf muscles and/or a flat arch in your foot. Other risk factors include running in worn out shoes, cold weather, frequently running uphill or if you suffer from medical conditions such as diabetes or high blood pressure. There are two main types of Achilles tendinitis: insertional and noninsertional. Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches to the heel bone. Noninsertional Achilles tendinitis is when the fibers in the middle portion of the tendon have started to break down with tiny tears, swell, and/or thicken. This type is more often seen in younger, active people. Both types can also cause bone spurs. Achilles tendonitis should be diagnosed by your doctor. However, if you experienced a sudden ?pop? in the back of your calf or heel, this might be something more serious like a ruptured or torn Achilles tendon. If this happens, see your doctor immediately.
If you have pain along the back of your leg near your heel, you may have Achilles tendonitis. Achilles tendonitis is an overuse injury that commonly occurs in runners and ?weekend warriors?. The Achilles tendon is the largest tendon in the body. Named after a tragic hero from Greek mythology, it connects your calf muscle to your heel bone to allow you to jump, run and walk. Achilles tendonitis is most common in middle-aged men, but it can happen to anyone who has a sudden increase in physical activity. The risk is increased if you also have tight calf muscles and/or a flat arch in your foot. Other risk factors include running in worn out shoes, cold weather, frequently running uphill or if you suffer from medical conditions such as diabetes or high blood pressure. There are two main types of Achilles tendinitis: insertional and noninsertional. Insertional Achilles tendinitis involves the lower portion of the heel, where the tendon attaches to the heel bone. Noninsertional Achilles tendinitis is when the fibers in the middle portion of the tendon have started to break down with tiny tears, swell, and/or thicken. This type is more often seen in younger, active people. Both types can also cause bone spurs. Achilles tendonitis should be diagnosed by your doctor. However, if you experienced a sudden ?pop? in the back of your calf or heel, this might be something more serious like a ruptured or torn Achilles tendon. If this happens, see your doctor immediately.
Causes
In some cases, Achilles Tendinitis can be caused by physical activity without a proper warm up or trauma, such as falling, to cause an overstressing of the muscle and tendon. Other causes include repetitive overuse syndrome, such as a job that required frequent heel lifting. Biomechanical causes such as pronation (or fallen arches) will cause the heel (calcaneus) to lean slightly, putting the undue stress on the Achilles tendon and the calf muscles. Most pain can be felt at the back of the heel or the point at which the calf muscle becomes a tendon three quarters of the distance down from the knee. Discomfort can be felt especially when jumping or when lifting the heel off the ground. Swelling and redness can often be seen at the back of the heel and touching the area would cause a tender sensation. In extreme cases, the tendon can become torn or rupture entirely which would cause bruising or an inability to put pressure on the foot.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
To diagnose the condition correctly, your doctor will ask you a few questions about the pain and swelling in your heel. You may be asked to stand on the balls of your feet while your doctor observes your range of motion and flexibility. The doctor may also touch the area directly. This allows him to pinpoint where the pain and swelling is most severe.
Nonsurgical Treatment
Make sure that the tendon is not torn through and through. If it is severed, you must see a doctor immediately so that the tendon can be repaired. Severe injuries can sever a tendon, without a skin laceration being present. Testing involves moving the toes and foot to see if the tendon moves. If the tendon does not appear to move, it may be severed (comparing the injured tendon and its movement to the same tendon on the uninjured foot may help). Very sharp pain, a sudden pop, or an obvious gap in the structure of the tendon are all signs of a rupture, and should be seen by a doctor as soon as possible. If there is extreme swelling of the leg, and pain (out of proportion to the amount of trauma received), you may have sustained a vascular injury. A doctor must see this type of injury immediately. If you are not sure, see a doctor. If you have multiple injured areas see a doctor immediately, in order to prevent excessive swelling and pain. If the above exam is negative, then you may proceed with self-treatment. (However, if you are not sure of the extent of your injury, you should consult your doctor immediately). The sooner you begin to treat your injury by following "R.I.C.E.", the better you will feel. Rest is very important. Take off your shoe, get off your feet, and relax. Ice should be applied as soon as possible. Never apply ice directly on the injured area, as the cold may make the pain worse. Ice should be applied close to the injured site, between the heart and the injury, so that as the blood flows under the ice, it will be cooled. This cool blood flowing into the injured area will help to reduce the swelling and pain. Apply the ice, wrapped in a cloth or over an elastic bandage, to the foot for 15 minutes, every 1-2 hours, for up to 3 days after an injury. If the ice is uncomfortable, or causes increased pain, do not continue to use it, and see a doctor. If you have poor circulation do not use ice, as this may cause a serious problem. c. Compression is used to limit swelling, and to give support to the injured area. Compression should be applied to the entire foot, starting first at the toes and working back to the ankle. If it is applied just to the injured area, increased swelling will occur in front and behind the wrapping. Compression should be applied with a 3-inch elastic bandage, beginning around the base of all the toes, and then going around the foot and ankle. Continue over the calf muscle when possible. Compression reduces motion in the injured area and foot, and this decreases the pain, and allows for quicker healing. The bandage should not be so tight that it causes increased pain or throbbing in the toes or foot. It should be comfortable! Do not remove the elastic bandage for the first 12 hours, unless it becomes too tight, or the pain increases, or the toes become pale, blue, or cool. If any of these things happen, immediately remove all bandages, and leave them off for several hours. The normal color and temperature of the toes should return immediately. If not, see a doctor immediately! Continue until the swelling and pain subsides; it could take from several days to several weeks. d. Elevation of the leg will aid in reducing swelling and pain. Blood rushes to an injured area to bring increased blood cells, that aid in healing. Gravity will also force blood to the injured area. Too many cells and too much fluid will apply pressure to the injured nerves and tissues, and cause increased pain and delayed healing. Keep your foot elevated so that it is at least parallel to the ground, or higher if it is comfortable. Do this for at least 48 hours, or until the throbbing subsides, when you lower the leg.

Surgical Treatment
Surgery is an option of last resort. However, if friction between the tendon and its covering sheath makes the sheath thick and fibrous, surgery to remove the fibrous tissue and repair any tears may be the best treatment option.
Prevention
Maintaining strength and flexibility in the muscles of the calf will help reduce the risk of tendinitis. Overusing a weak or tight Achilles tendon makes you more likely to develop tendinitis.
What Can You Do About Achilles Tendonitis ?
Overview
 Achilles tendinitis. Achilles tendonitis is inflammation of the Achilles tendon, the largest tendon in the body, which runs from the calf to the heel bone. Noninsertional Achilles tendonitis affects fibers in the middle of the tendon. Insertional Achilles tendonitis affects the lower portion of the tendon where it attaches to the heel bone. Both types can result from repetitive stress to the tendon or from overstressing the tendon during exercise. Damaged tendon fibers can calcify and bone spurs can form where the tendon attaches to the bone. Symptoms may include pain and stiffness of the tendon - which may occur from either inactivity (such as first thing in the morning) or after activity - thickening or swelling of the tendon or bone spurs.
Achilles tendinitis. Achilles tendonitis is inflammation of the Achilles tendon, the largest tendon in the body, which runs from the calf to the heel bone. Noninsertional Achilles tendonitis affects fibers in the middle of the tendon. Insertional Achilles tendonitis affects the lower portion of the tendon where it attaches to the heel bone. Both types can result from repetitive stress to the tendon or from overstressing the tendon during exercise. Damaged tendon fibers can calcify and bone spurs can form where the tendon attaches to the bone. Symptoms may include pain and stiffness of the tendon - which may occur from either inactivity (such as first thing in the morning) or after activity - thickening or swelling of the tendon or bone spurs.
Causes
Excessive exercise is a common cause of Achilles tendonitis. This is particularly true for athletes. However, factors unrelated to exercise may also contribute to risk. Rheumatoid arthritis and infection are both correlated with tendonitis. In general, any repeated activity that strains the Achilles tendon can contribute to this problem. Here are a few possible causes, jumping into an exercise routine without a proper warm-up, straining calf muscles during repeated exercise or physical activity, playing sports such as tennis that require quick stops and changes of direction, wearing old or ill-fitting shoes, wearing high heels every day.
Symptoms
Symptoms can vary from an achy pain and stiffness to the insertion of the Achilles tendon to the heel bone (calcaneus), to a burning that surrounds the whole joint around the inflamed thick tendon. With this condition, the pain is usually worse during and after activity, and the tendon and joint area can become stiffer the following day. This is especially true if your sheets are pushing down on your toes and thereby driving your foot into what is termed plantar flexion (downward flexed foot), as this will shorten the tendon all night.
Diagnosis
A doctor or professional therapist will confirm a diagnosis, identify and correct possible causes, apply treatment and prescribe eccentric rehabilitation exercises. An MRI or Ultrasound scan can determine the extent of the injury and indicate a precise diagnosis. Gait analysis along with a physical assessment will identify any possible biomechanical factors such as over pronation which may have contributed to the achilles tendonitis and training methods will be considered. Biomechanical problems can be corrected with the use of orthotic inserts and selection of correct footwear.
Nonsurgical Treatment
If caught early enough, simple physical therapy that you can do by yourself should be fine. Over the counter solutions as easy as pain medication, cold compresses, a different pair of shoes, or a new set of stretching exercises can make most of the symptoms of Achilles tendinitis disappear. Further trouble or extreme pain should be regarded as a sign that something more serious is wrong, and you should immediately consult a doctor or physician. They will look to see whether non-surgical or surgical methods are your best options, and from there you can determine what your budget is for dealing with the condition.

Surgical Treatment
Surgery is considered the last resort and is often performed by an orthopedic surgeon. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
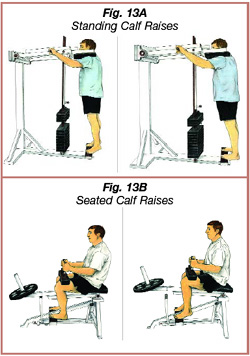
Regardless of whether the Achilles injury is insertional or non-insertional, a great method for lessening stress on the Achilles tendon is flexor digitorum longus exercises. This muscle, which originates along the back of the leg and attaches to the tips of the toes, lies deep to the Achilles. It works synergistically with the soleus muscle to decelerate the forward motion of the leg before the heel leaves the ground during propulsion. This significantly lessens strain on the Achilles tendon as it decelerates elongation of the tendon. Many foot surgeons are aware of the connection between flexor digitorum longus and the Achilles tendon-surgical lengthening of the Achilles (which is done to treat certain congenital problems) almost always results in developing hammer toes as flexor digitorum longus attempts to do the job of the recently lengthened tendon. Finally, avoid having cortisone injected into either the bursa or tendon-doing so weakens the tendon as it shifts production of collagen from type one to type three. In a recent study published in the Journal of Bone Joint Surgery(9), cortisone was shown to lower the stress necessary to rupture the Achilles tendon, and was particularly dangerous when done on both sides, as it produced a systemic effect that further weakened the tendon.
Achilles Tendon Rupture Fallacies
Overview

The Achilles tendon is the largest tendon in the human body. It connects the calf muscle to the heel bone. However, this tendon is also the most common site of rupture or tendonitis, an inflammation of the tendon due to overuse. Achilles tendon rupture is a partial or complete tear of the Achilles tendon. It comes on suddenly, sometimes with a popping sound, and can be debilitating. A full rupture is more severe, but less common, than a partial rupture. A full rupture splits the Achilles tendon so that it no longer connects the calf muscle to the heel: the calf muscle can no longer cause the foot to ?push off?, so normal walking is impossible. If it is a full rupture, then lightly pinching the Achilles tendon with the forefinger and thumb will reveal a gap in the Achilles tendon. Partial and full Achilles tendon ruptures are most likely to occur in sports requiring sudden stretching, such as sprinting and racquet sports. Partial Achilles tendon tears are also common among middle and long distance runners.
Causes
Your Achilles tendon helps you point your foot downward, rise on your toes and push off your foot as you walk. You rely on it virtually every time you move your foot. Rupture usually occurs in the section of the tendon located within 2.5 inches (6 centimeters) of the point where it attaches to the heel bone. This section may be predisposed to rupture because it gets less blood flow, which may impair its ability to heal. Ruptures often are caused by a sudden increase in the amount of stress on your Achilles tendon. Common examples include increasing the intensity of sports participation, falling from a height, stepping into a hole.
Symptoms
Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel, an inability to bend your foot downward or "push off" the injured leg when you walk, an inability to stand on your toes on the injured leg, a popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward.
Diagnosis
The doctor may look at your walking and observe whether you can stand on tiptoe. She/he may test the tendon using a method called Thompson?s test (also known as the calf squeeze test). In this test, you will be asked to lie face down on the examination bench and to bend your knee. The doctor will gently squeeze the calf muscles at the back of your leg, and observe how the ankle moves. If the Achilles tendon is OK, the calf squeeze will make the foot point briefly away from the leg (a movement called plantar flexion). This is quite an accurate test for Achilles tendon rupture. If the diagnosis is uncertain, an ultrasound or MRI scan may help. An Achilles tendon rupture is sometimes difficult to diagnose and can be missed on first assessment. It is important for both doctors and patients to be aware of this and to look carefully for an Achilles tendon rupture if it is suspected.
Non Surgical Treatment
There are two treatment options available which are non-operative and operative. Non-operative treatment involves the use initially of a below-knee plaster with the foot held fully bent downwards. This usually stays in place for 2 weeks then is changed for a brace(this is a boot from the knee down to the toes with Velcro straps) which should be worn day and night. The brace will be regularly altered to allow the foot to come up to a more neutral position. The brace will be on for a further 6 weeks. After the 8 weeks you will be referred for physiotherapy to regain movement and calf strength but will probably need to wear the brace during the day for a further 4 weeks. Non-operative treatment avoids the risks of surgery but the risk of the tendon re-rupturing, which normally occurs within 3 months of discarding the brace, is 10%.

Surgical Treatment
There are two types of surgery to repair a ruptured Achilles tendon. In open surgery, the surgeon makes a single large incision in the back of the leg. In percutaneous surgery, the surgeon makes several small incisions rather than one large incision. In both types of surgery, the surgeon sews the tendon back together through the incision(s). Surgery may be delayed for about a week after the rupture, to let the swelling go down.
About
Fashion is in my blood. When I was a kid, my mom would drive me two hours through crazy LA traffic for photo shoots. I used to hang out with the stylists, try on clothes, get advice. It was a great way to grow up. Eventually, I started giving my friends fashion advice, and never looked back.
After 20 years as a stylist for photographers, I was ready to start a business that would let me evolve my own fashion and consulting style. More than anything, I wanted to share my passion for fashion, and watch as my clients discovered the transformative power of a knock-out look.
Today my clients are CEOs, celebrities, corporate and creative people -- men and women who want serious input on their clothing style, advice on what to wear to an event, or how to put together and pack the most versatile travel wardrobe. I also do styling for fashion shoots, including art direction, makeup, hair, clothing and accessorizing. I’ll make you look great. I promise.